| Chronic obstructive pulmonary disease (COPD) |
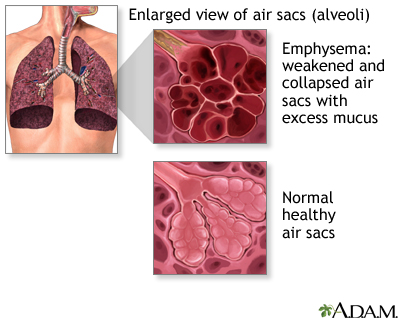
Chronic obstructive pulmonary disease (COPD) refers to chronic lung disorders that result in blocked air flow in the lungs. The two main COPD disorders are emphysema and chronic bronchitis, the most common causes of respiratory failure. Both result from damage to the lungs over many years and predominantly affect former and current smokers. Emphysema occurs when the walls between the lung's air sacs become weakened and collapse. Chronic bronchitis occurs when the airways in the lungs become swollen and partially clogged with mucus. Chronic bronchitis may also involve muscle spasms in the airways. Many people with COPD have both emphysema and chronic bronchitis.
According to the American Lung Association, COPD is the fourth leading cause of death in the United States, with over 11 million Americans diagnosed with it (and probably at least that many who have it and are not diagnosed), and over 120,000 Americans dying from it annually (beginning in 2002, more women than men). Asthma and COPD are considered different medical problems. Patients with COPD may also wheeze. The damage to the airways from COPD usually is more permanent and irreversible.
"I was so scared when I first learned I had COPD. I had no idea what it was, much less what to expect or how to cope." -- Charlie, age 72 |
What causes COPD?
Tobacco smoking is the most common cause of COPD, accounting for 80 - 90% of COPD deaths. Women smokers are nearly 13 times as likely to die from COPD as are women who have never smoked. Men smokers are nearly 12 times as likely to die from COPD as men who have never smoked. Cigarettes contain many hazardous substances that damage the lung when inhaled, including tar nicotine, carbon monoxide, and cyanide. Long-term exposure to secondhand tobacco smoke, air pollution, and repeated respiratory infections also can increase a person's risk for COPD. Industrial exposures, such as toxic fumes or dust, can significantly increase a person's risk of COPD as well.

What are the symptoms?
COPD has three main symptoms: coughing, breathlessness, and wheezing.
COPD is often diagnosed in the doctor's office when patients complain of difficulty breathing while doing everyday tasks or complain of a persistent cough. COPD patients often cough up thick or bloody mucus, and their skin may have a bluish tinge caused by lack of oxygen in the blood. If patients develop severe shortness of breath or swelling of the legs or ankles, they require immediate attention, as these symptoms may signify congestive heart failure.
How does a doctor make a diagnosis of COPD?
Although a definite diagnosis of COPD can be difficult, doctors rely on certain assessment procedures to help them diagnose the condition. Your doctor may:
- Ask the following questions about your health history
- What is your smoking history?
- Do you suffer from shortness of breath?
- What worsens your shortness of breath?
- Do you cough?
- Do you cough up mucus, and if so, what does it look like?
- What is your family history of lung disease?
- Conduct a spirometry test -- this test is a common and effective way to test your lungs. Your doctor will ask you to blow as long and as hard as you can into a small tube attached to a machine. The machine measures how much air you can blow out in one second. The more obstructed the airways, the less air you can blow out.
- Order blood tests and chest x-rays -- blood tests measure the amount of oxygen and carbon dioxide in your blood, which denote how efficiently your lungs are working. Chest x-rays can help determine if there is fluid in the lungs or other damage.
How is COPD treated?
Although the damage caused by emphysema is irreversible, some of the effects of chronic bronchitis can be partially improved. The progression of COPD and the severity of the symptoms might be managed through the following methods:
- Bronchodilators -- can be administered as pills, liquids, or inhalers. They open up the air passages in the lungs.
- Antibiotics -- COPD reduces the effectiveness of the lungs' natural defense systems. Antibiotics can get rid of bacterial infection in the lungs when they are in this compromised state.
- Pulmonary rehabilitation -- a pulmonary rehabilitation program is provided by a team of health professionals to help COPD patients cope physically, psychologically, and socially with the disease. The program strives to help patients achieve the highest possible quality of life within the limitations of the disease.
- Oxygen -- for severe cases of COPD, supplemental oxygen, using a tank and face mask, may be necessary.
- Fluid clearing device -- The Flutter device is a small, drug-free unit designed to help patients easily cough out the extra fluid in their lungs.
- Lung transplantation
- Lung volume reduction surgery (LVRS)
Prevention
- Avoid smoking tobacco or exposure to secondhand tobacco smoke. Smoking is the leading cause of COPD. Although you cannot undo the damage that smoking has already caused, you can prevent further lung damage by quitting.
- Decrease exposure to environmental irritants. Irritants such as secondhand smoke, strong odors, and fumes can lead to further narrowing of the airways in the lungs. COPD patients should avoid breathing the fumes from perfume, paints, and cleaning supplies.
- Use appropriate protective gear (e.g. face mask) in the workplace to avoid inhaling hazardous substance.
- Get plenty of physical activity for good lung health.
- If you already have COPD, avoid colds, pneumonias, and flus, which can worsen the disease. Get pneumococcal and annual flu vaccinations to avoid such infections.
Reference
American Lung Association: Chronic Obstructive Pulmonary Disease (COPD) Fact Sheet (Chronic Bronchitis and Emphysema). 2006 August.
Reviewed By: Allen J. Blaivas, DO, Clinical Assistant Professor of Medicine UMDNJ-NJMS, Attending Physician in the Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Veteran Affairs, VA New Jersey Health Care System, East Orange, NJ. Review provided by VeriMed Healthcare Network. Previoulsy reviewed by David A. Kaufman, MD, Section Chief, Pulmonary, Critical Care & Sleep Medicine, Bridgeport Hospital-Yale New Haven Health System, and Assistant Clinical Professor, Yale University School of Medicine, New Haven, CT. Review provided by VeriMed Healthcare Network. (6/1/2010)
 All rights reserved.
All rights reserved.